Appendix C National Validation Study
Defining and Measuring the Competence of Addiction Counselors
Paula K. Horvatich, Ph.D., and Jon F. Wergin, Ph.D. Virginia Commonwealth University[1]
Introduction
The education of addiction counselors, once based on tradition, myth, and politics, is becoming increasingly professionalized, based on competencies, research, and best practice (Fisher 1997). Treatment for psychoactive substance abuse and dependence has traditionally been provided by addiction counselors. Although many counselors have academic degrees, many others have become counselors following personal experiences with treatment and recovery (Deitch & Carleton 1997). Formal education for addiction counselors has traditionally consisted of specialty training provided by treatment agencies, professional or certification organizations, or human service programs of community colleges that confer associate’s degrees. Certification of addiction counselors varies from State to State but usually requires a high school diploma and a specified number of years of experience in the field. A bachelor’s degree is required in only some States. In others, addiction counselors require no certification as long as they work in a State-approved facility.
Because of a variety of policy and economic factors, training requirements for certification in addiction counseling have become more rigorous. These factors include, among others, the pervasiveness and effect of substance abuse on society, expanded treatment research efforts, and managed behavioral health care. If substance use problems were not so widespread and costly to society, there would be less interest in the credentials of addiction counselors and the outcomes of the treatment they provide.
Although treatment research has grown rapidly and has provided useful insights, new informa- tion will be useless unless it is implemented by frontline practitioners. Addiction counselors must be able to understand and apply new knowledge, but traditionally these connections have not been made (Fisher 1997).
Efforts to make treatment more efficient have resulted in the integration of substance abuse treatment with mental health services, thereby increasing the role of mental health and other healthcare professionals in substance abuse treatment. Addiction specialties have emerged in medicine, nursing, social work, psychology, and counseling, including rehabilitation counseling. Managed care has made it increasingly likely that master’s-level addiction counselors will be reimbursed for services provided. Addiction counselors who are currently certified with only a high school diploma may have difficulty making the leap to a master’s degree. Many addiction counselors may not be able to obtain the advanced education needed fast enough to survive in the market.
In 1993 the Center for Substance Abuse Treatment (CSAT) created the Addiction Technology Transfer Center (ATTC) Program to foster improvements in the preparation of addiction treatment professionals (Rohrer et al. 1996). As part of the ATTC Program, a National Curriculum Committee (the Committee) was established to evaluate existing curricula and to set priorities for current academic programs. At its first meeting, the Committee realized that the field had not defined the knowledge, skills, and attitudes that should be shared by all addiction counselors. Identifying and delineating these competencies became the Committee’s first task to professionalize the field.
Representing a range of specialties within the substance abuse treatment field, members of the Committee provided practice-related information through a brainstorming process. Once the general responsibilities of the field were identified, the Committee developed task statements for each. Committee members ordered the responsibilities and task statements in a learning sequence, based on the order in which responsibilities are generally performed on the job. The process of identifying responsibilities was considered complete when the Committee reached consensus regarding the accuracy and sequence of the task statements produced. The Committee identified four transdisciplinary foundations and eight practice dimensions encompassing 121 competencies. These results are consistent with the DACUM (Develop a Curriculum) process (Norton 1985), which typically results in 8 to 12 responsibilities and 50 to 200 tasks. The four transdisciplinary foundation categories were understanding addiction, treatment knowledge, application to practice, and professional readiness. The eight practice dimension categories were clinical evaluation; treatment planning; referral; case management; counseling; client, family, and community education; documentation; and professional and ethical responsibilities. Each category had between 3 and 20 competencies in it. This effort resulted in the publication of Addiction Counselor Competencies (Addiction Technology Transfer Centers 1995).
Although the Committee incorporated existing literature related to the work of addiction counselors, particularly the practice analysis conducted by Birch and Davis Corporation (1986) and the International Certification and Reciprocity Consortium Role Delineation Study (International Certification and Reciprocity Commission/Alcohol and Other Drug Abuse 1991) when developing the competencies that made up Addiction Counselor Competencies, it also relied on its own contributions. The Committee felt that job-related data provided a snapshot of what is, not what could be. And in the addiction counseling field, what is has been questioned. Because of its peer counselor and personal experience history, treatment provided by some addiction counselors has been described as narrow and inflexible, impeding the adoption of new treatment methods that may better meet the needs of clients. Moreover, lacking traditional academic preparation, some counselors have difficulty understanding literature and incorporating new research results. Consequently, the Committee’s work emphasized moving the field forward. To gauge the potential value of the competencies, the Committee conducted a study to determine which of 121 competencies were perceived as necessary for practice by addiction counselors in the field.
Method
The purposes of this study were the following:
- Validate a set of 121 competencies for the profession of addiction counseling
- Determine gaps between actual and needed competencies displayed by entry-level counselors
- Determine congruence among the perceptions of three practitioner groups.
The study was conducted in partnership with the ATTCs, CSAT, and the Northwest Regional Educational Laboratory (Adams & Gallon 1997).
A survey was conducted in 16 States and Puerto Rico from November 1996 to January 1997. The survey instrument was distributed through the ATTCs to State-approved substance abuse treatment agencies. State authorities worked with ATTCs to select qualified treatment sites, distribute the surveys with appropriate cover letters from the State authority, and implement followupstrategies to ensurean adequate return rate.
A random sample of 60 State-approved treatment facilities was selected in each participating State. For States with fewer than 60 qualifying facilities, all State-approved treatment facilities were included in the study, if the facilities were large enough to have a separate clinical supervisor who was not also an administrator in the facility.
Each treatment agency director was sent a cover letter and instructions, three copies of the 16-page survey listing 121 competencies, and corresponding postage-paid return envelopes.
Directors were asked to distribute the surveys to a clinical supervisor, a least experienced counselor, and a most proficient counselor. “Least experienced” was defined as nonsupervisory, direct-care counselors having no more than 3 years of paid experience as an addiction treat- ment professional. Each respondent rated the level of proficiency “typically demonstrated” by entry-level counselors at the time of hire, as well as the level of competency “needed” at the time of hire. Each respondent was instructed to provide a rating for each item on a five-point scale, ranging from 1 (“very little to no knowledge/skill/attitude”) to 5 (“excellent knowledge/skill/ attitude”). Beginning 1 week following the due date of the responses, telephone calls were placed with nonresponding agencies, encouraging them to submit finished surveys. Final response rates varied by State, ranging from 25 percent in North Carolina to 82 percent in Maryland; the response rate nationally was 46 percent. The total number of respondents was 1,238.
Results
Demographics. (See exhibits 1–6.) Respondents included 369 least experienced counselors, 412 most proficient counselors, and 457 clinical supervisors (N=1,238). Females outnumbered males in all respondent groups. The sample was mostly middle-aged, and age increased with level of experience. Seventy-five percent of the respondents were Caucasian, 14 percent African American, 7 percent Hispanic, and 4 percent filled other minority categories or were undeclared.
The respondents were well educated with 74 percent reporting bachelor’s or master’s degrees. As expected, clinical supervisors reported the greatest number of graduate degrees. Clinical supervisors and most experienced counselors reported the longest employment in the field (i.e., more than 5 years). Although “least experienced” was defined as no more than 3 years’ paid experience, many “least experienced” counselors reported more than 3 years of employment in the addiction profession. This may be the result of a mistaken inclusion of other experiences in the field such as volunteer service, internships, or personal treatment and recovery. The least experienced counselors had the smallest proportion certified, whereas clinical supervisors had the highest proportion certified.
Data reduction procedures. Given the huge number of possible cross-tabulations with a survey this size, results have been summarized in three different ways. First, because the pur-pose of the study was to identify “essential” competencies, survey responses were collapsed into percentages of respondents rating each item “4” or “5” (“good” or “excellent”). Excluding the “moderate” ratings provides a more stringent standard for judging the content validity of the competencies. Second, results were provided for the national sample only. Third, responses were summarized across individual competencies within the 12 competency categories.
Validation of the 121 competencies. Internal consistency of the survey was high: Cron-bach’s Alpha for the 12 sections of the survey ranged from 0.91 to 0.98. Among the clinical supervisors, 40 percent of respondents indicated that entering practitioners needed to be “good” or “excellent” in all 121 competencies; 60 percent gave these ratings for 118 of the 121 compe-tencies; and 70 percent gave these ratings for 107 of the 121 competencies. Clearly, the surveyed competencies had high content validity for these experienced practitioners.
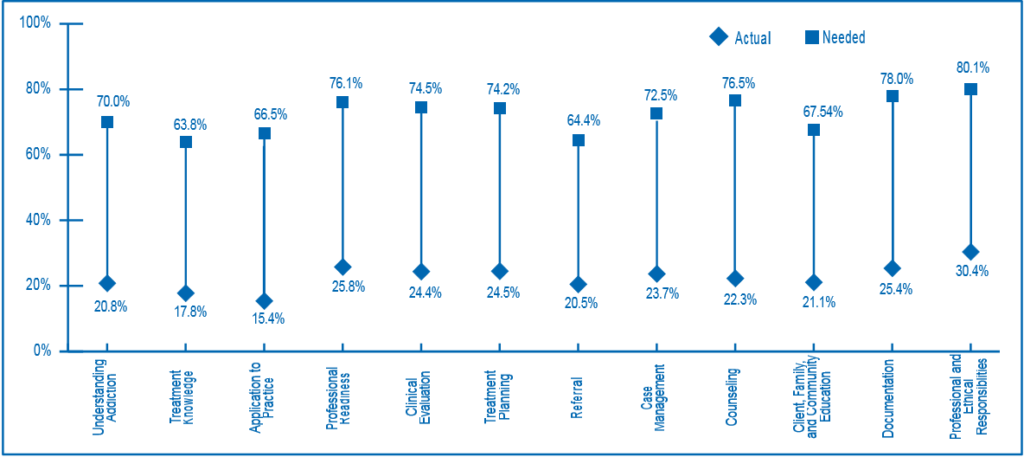
Gaps between actual and needed competencies. Large differences were found between perceived needed and actual proficiency, across all three respondent groups. As exhibit 7 indi-cates, the gap was most pronounced among clinical supervisors. For all but 1 of the 121 items, less than half the supervisors rated actual proficiencies as “good” or “excellent.” Exhibit 8 displays the percentage gaps for each of the 12 categories, as reported by clinical supervisors only. Gaps between actual and needed proficiencies are evident across categories, ranging from a 44-percent gap for the “Referral” category to a 54-percent gap for the “Counseling” category. Just as the perceived need for counselor competencies was consistently high, the perceived level of actual competencies was consistently low.
Congruence among perceptions of counselor groups. As exhibit 7 indicates, although the three counselor groups are consistent with one another in their ratings of need, they differ consistently in their ratings of actual proficiency. In each category the lowest ratings were given by supervisors, followed by “most proficient” and then “least experienced” counselors. Differ-ences between supervisors and least experienced counselors were lowest in the “Treatment Planning” category and greatest—not surprisingly—in the “Professional Readiness” category.
Competency subsets. Ratings of some subsets of the competencies indicate a need for further study. For example, supervisors and counselors seemed to undervalue competencies related to research and treatment outcome assessment. The Committee included these compe-tencies because it felt that the counselors’ abilities to assess and monitor outcomes and apply research findings to their own practices were important and would contribute to the profession-alization of the field.
In sum, this survey revealed large and consistent gaps between actual and needed competencies across all categories, with clinical supervisors perceiving the largest differences.
Discussion
Clinical supervisors, entry-level counselors, and most proficient counselors endorsed almost all 121 competencies as important. However, the responses of each professional group also show relatively little discrimination among items and categories, which may account for the high Alpha coefficients. Given the large number of items in the survey, this level of consistency could indicate a substantial halo effect: that is, respondents could have been answering individual items on the basis of an overall impression and not making fine discriminations among the individual competencies.
The results also indicate large gaps between what is needed and observed in proficiency for entry-level counselors, even among entry-level counselors themselves. Supervisors noted the greatest gaps, followed by the most proficient and entry-level counselors. Although the least ex- perienced counselors reported the smallest gaps, the gaps were still substantial, indicating that what counselors know they need to do the job and what they can do are two different things.
What accounts for supervisors’ ratings of entry-level proficiency being more critical than the other respondent groups? One possibility is a contrast effect. That is, supervisors may be us- ing their own level of expertise as the standard for comparison resulting in unrealistically high expectations for entry-level counselors. In this instance, counselors with average proficiency would receive lower ratings against the supervisors’ higher standard representing significantly more experience.
As a content validation strategy, the survey has limited value. Respondents were given 121 statements to respond to, and little discrimination among the items was observed. However, all the competencies were perceived to be important, and the preparation for each was always reported as inadequate. Respondents appeared to address the list as a whole, rather than the individual competencies. Those who would embark on curricular change should do the same. That is, formal preparation for addiction counselors cannot just be bolstered here and there; it needs to be comprehensively redesigned.
The main benefit of the survey results may be as a catalyst for curricular change. This has already proven to be the case. While the survey was being conducted, the Committee was already working on an expanded document that listed the knowledge, skills, and attitudes for each of the 121 competencies. Feedback from the field was obtained on the draft document. Then the International Certification and Reciprocity Consortium (ICRC) convened a national leadership group to assess the need for model addiction counselor training. After careful deliberation, the group concluded that much of the work to define such a curriculum standard had already been accomplished by the Committee and the ICRC in the Committee’s Addiction Counselor Compe- tencies and the ICRC’s 1996 Role Delineation Study, respectively.
Soon after, CSAT agreed to fund a collaborative effort to finalize a document that could be used as a national standard. CSAT convened a panel—The National Steering Committee for Addiction Counseling Standards (NSC)—that comprised representatives from five national educational, certification, and professional associations. The NSC was successful in achieving unanimous endorsement of the Addiction Counselor Competencies—a milestone in the addiction counsel- ing field. In 1998 CSAT published the results of this groundbreaking work as TAP 21: AddictionCounseling Competencies: The Knowledge, Skills, and Attitudes of Professional Practice.
The significance of TAP 21 for addiction counseling was that it provided a single frame of reference for curriculum development, student advising, professional development, and clinical supervision. The current updated edition of TAP 21 continues the work of furthering the professionalization of the addiction counseling field.
Conclusions
Although this is a study of perceptions and professional judgment and further inquiry is needed into the reasons for the discrepancies, these results suggest that clinical supervisors are getting far less than they need in entry-level counselors. More systematic discussions between clinical practitioners and faculty of training programs in addiction counseling should produce a redefinition of curricular goals based on the competencies described in this document.
Addiction counseling is a profession in the making. Rather than maintaining its professional culture by relying on tradition, addiction counseling is building its identity from the ground up, by first identifying competencies all addiction counselors are expected to possess. Such an approach addresses directly the “education–practice discontinuity” cited by Cavanaugh (1993) as one of the most critical problems in professional education.
References
Adams, R.J., & Gallon, S.L. (1997). Entry Level Addiction Counselor Competency Survey: National Results. Portland, OR: Northwest Regional Educational Laboratory.
Addiction Technology Transfer Centers, National Curriculum Committee (1995). Addiction Counselor Competencies. Rockville, MD: Center for Substance Abuse Treatment.
Birch and Davis Corporation (1986). Development of Model Professional Standards forCounselor Credentialing. Dubuque, IA: Kendall/Hunt Publishing.
Cavanaugh, S.H. (1993). Connecting education and practice. In L. Curry & J.F. Wergin (Eds.) Educating Professionals. San Francisco: Jossey-Bass.
Deitch, D.A., & Carleton, S.A. (1997). Education and training of clinical personnel. In J.H. Lowinson, P. Ruiz, et al. (Eds.) Substance Abuse: A Comprehensive Textbook. Baltimore, MD: William & Wilkins.
Fisher, G. (September 1997). Training Issues for Addiction Counselors and Other Helping Professions. Paper presented at the meeting of the Mid-Atlantic Addiction Educator’s Conference, Williamsburg, VA.
International Certification and Reciprocity Consortium/Alcohol and Other Drug Abuse (1991). Role Delineation Study for Alcohol and Other Drug Abuse Counselors. Raleigh, NC: National Certification Reciprocity Consortium/Alcohol and Other Drug Abuse.
Norton, R.E. (1985). DACUM Handbook. Columbus, OH: Ohio State University National Center for Research in Vocational Education.
Rohrer, S.R., Diesenhaus, D.I., et al. (1996). Addiction Technology Transfer Centers (ATTCs). Substance Abuse, 4:193-199.
Exhibits (Adams and Gallon 1997)
Adams, R.J., & Gallon, S.L. (1997). Entry Level Addiction Counselor Competency Survey: National Results. Portland, OR: Northwest Regional Educational Laboratory.
Exhibit 1. Gender
|
Gender |
Supervisor |
Most Proficient | Least Experienced |
Total |
| Male | 198 | 153 | 130 | 481 |
| Female | 259 | 259 | 239 | 757 |
| TOTAL | 457 | 412 | 369 | 1,238 |
Exhibit 2. Age
|
Age |
Supervisor |
Most Proficient | Least Experienced |
Total |
| <21 | 0 | 0 | 1 | 1 |
| 21–29 | 19 | 30 | 72 | 121 |
| 30–39 | 104 | 112 | 106 | 322 |
| 40–49 | 194 | 169 | 118 | 481 |
| 50–59 | 115 | 79 | 53 | 247 |
| 60+ | 17 | 18 | 15 | 50 |
| TOTAL | 449 | 408 | 365 | 1,222 |
Exhibit 3. Race/ethnicity
| Race/Ethnicity | Supervisor | Most Proficient | Least Experienced | Total |
| African American | 60 | 56 | 57 | 173 |
| Hispanic | 28 | 32 | 31 | 91 |
| White | 345 | 305 | 262 | 912 |
| Native American | 5 | 8 | 5 | 18 |
| Asian/Pacific Islander | 3 | 1 | 2 | 6 |
| Other | 7 | 1 | 1 | 9 |
| Undeclared | 5 | 5 | 4 | 14 |
| TOTAL | 453 | 408 | 362 | 1,223 |
Exhibit 4. Education
| Education | Supervisor | Most Proficient | Least Experienced | Total |
| GRE/high school diploma | 9 | 6 | 13 | 28 |
| Some college or technical/trade school | 50 | 65 | 70 | 185 |
| Associate’s degree | 23 | 49 | 37 | 109 |
| Bachelor’s degree | 112 | 130 | 135 | 377 |
| Graduate degree (master’s level and above) | 257 | 161 | 110 | 528 |
| TOTAL | 451 | 411 | 365 | 1,227 |
Exhibit 5. Period of Employment in the Addictions Profession
| Employment History | Supervisor | Most Proficient | Least Experienced | Total |
| Less than 6 months | 4 | 10 | 30 | 44 |
| 6 months to 18 months | 13 | 17 | 78 | 108 |
| 19 months to 3 years | 20 | 31 | 68 | 119 |
| 3 to 5 years | 49 | 67 | 69 | 185 |
| 5 to 10 years | 113 | 159 | 80 | 352 |
| More than 10 years | 251 | 126 | 40 | 417 |
| TOTAL | 450 | 410 | 365 | 1,225 |
Exhibit 6. Addictions Certification
| Certificate Status | Supervisor | Most Proficient | Least Experienced | Total |
| Certified | 308 | 264 | 156 | 728 |
| Not certified | 144 | 141 | 209 | 494 |
| TOTAL | 452 | 405 | 365 | 1,222 |
Exhibit 7. Ratings of actual vs. Needed proficiency
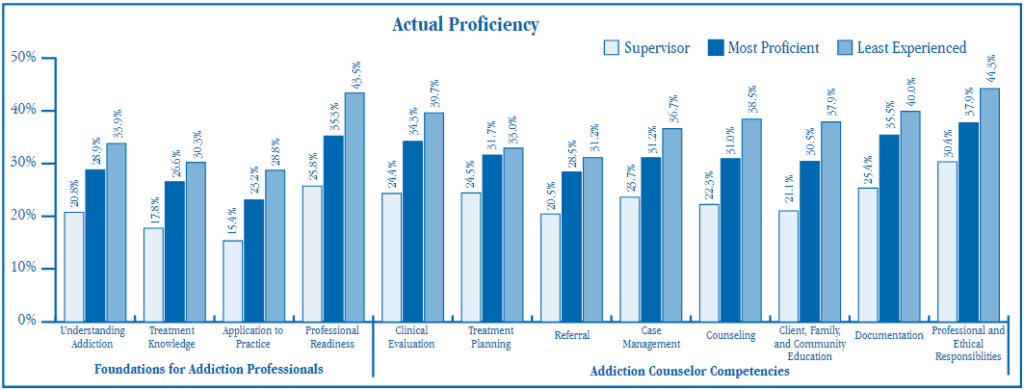
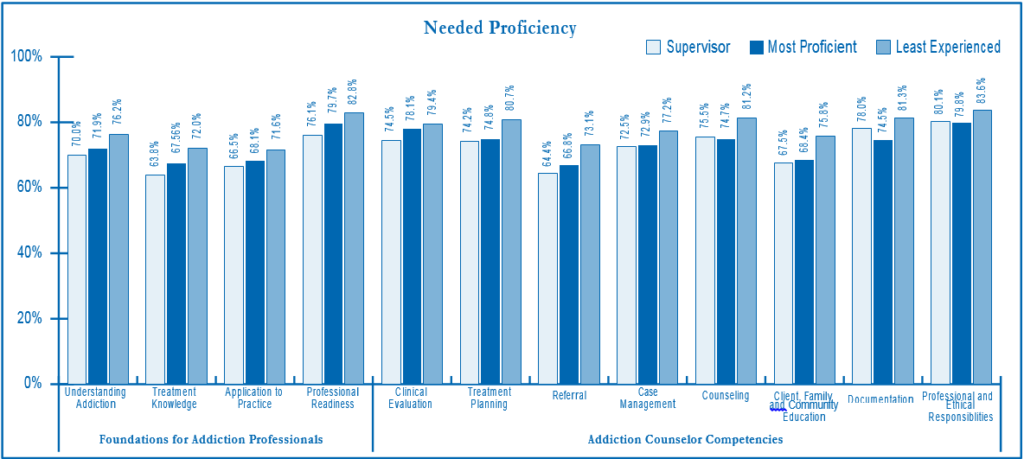
Exhibit 8. Percentage gap between actual and needed level as perceived by supervisors
- An earlier version of this paper was presented at the American Educational Research Association Annual Meeting, April 13–17, 1998, in San Diego, California. This study was funded by the Substance Abuse and Mental Health Services Administration’s Center for Substance Abuse Treatment Grant Number 5U98 TI 00837. The original version is archived on the Education Resources Information Center (ERIC) Web site under ERIC document number ED422545. ↵
